 Preventing Heart Attacks with Ouabain
Reversing Heart Disease Part Five
Preventing Heart Attacks with Ouabain
Reversing Heart Disease Part Five
by Jeffrey Dach MD
Our previous articles in this series,
Parts one,
two,
three and
four
have made the case for the "clogged artery" filled with atherosclerotic
plaque as the cause for heart attacks. Indeed, imaging studies and
autopsy studies show extensive arterial plaque formation in the
unfortunate victims of heart attacks.
Above left image Strophanthus Flower source for Ouabain, Cardiac Drug. Courtesy of wikimedia commons.
The Plumbing Approach to Heart Disease

Recognizing
the "clogged artery" as the cause of heart attacks, we have built an
entire medical industry devoted to unclogging them with the "plumbing
approach". Heroic doctors serve as glorified plumbers, advancing
catheters, angioplasty balloons and stents into the patient to open up
these clogged arteries. If the catheters, balloons, and stents fail,
the open-heart bypass operation is next. For those patients who escape
the attention of the invasive cardiologist with their heroic plumbing
procedures, there is "medical treatment" with cardiac drugs such as
Statins, Beta Blockers, Calcium Channel blockers, Nitrates, Aspirin,
blood thinners etc .
Left image: Cardiac Bypass Operation, opening up clogged arteries with a bypass.

According
to mainstream cardiology, heart attacks are caused by obstruction of
the coronary artery shutting off oxygen supply to a segment of the heart
muscle which then undergoes "infarction", a word meaning cell death
from lack of oxygen. No doubt this does happen in most but not all
cases.
Above Left Image : Plumber Opening Clogged Pipe similar to our current medical procedures. Courtesy of Wikimedia Commons.
What Causes Heart Attacks ?
Heart Attack with Normal Coronary Arteries - Clogged Arteries with No Heart Attack

We know that in some
cases, heart attacks occur with completely normal coronary arteries as demonstrated by angiography or autopsy examination.(25-31).
Not only that,
autopsy studies on young trauma victims show left main or multivessel disease in 20%, yet heart attacks are rare in this age-group.
Autopsy studies
of hospitalized patients who die of non-cardiac causes show 41% have
critical stenosis or occlusion of at least one major vessel. Why
didn't they die of a heart attack first ? Clearly there must be other
factors at work. Clogged arteries are quite common and some people seem
to do Ok with it. We will pick up this idea later.
Left Image: Coronary arteries courtesy of wikimedia commons.
Coronary Artery Theory
In
the Coronary Artery Theory of Heart Attacks, the arterial plaque
continues to enlarge causing narrowing of the arterial lumen
(stenosis). This stenosis is like closing a water faucet reducing blood
flow down to a trickle. Finally, the "ruptured plaque" is the final
event triggering thrombosis and total obstruction of the coronary
artery. Downstream from the blocked artery, the heart segment
undergoes cell death from lack of oxygen. This is called a myocardial
infarction, or heart attack.
The Zipper Club

This
Coronary Artery Theory is the working hypothesis of the mainstream
cardiologist who would never question it, and happily goes about his job
as a glorified pumber, searching out all the clogged arteries with
imaging in the cath lab. His job is to inject radiographic dye into the
coronary arteries looking for the stenosis. If a severely narrowed
artery is discovered, the invasive cardiologist will promptly perform a
plumbing procedure, the angioplasty or stent to open the narrowed
artery. If this is proves to be unsuccessful, the patient may be sent
next door to the surgical department. They may wake up in the recovery
room after a "Cabbage" , a (CABG) Coronary Artery Bypass Graft. This
is also called the "
Big Zipper" and Zipper Club tee shirts are available
(left image courtesy of Mended Little Hearts of Winchester.)
A
massive medical industry has been built on the Coronary Artery Theory
of heart disease. Your local hospital might very well be in an
expansion phase, building larger facilities to do all this.
Left Image: Construction Cranes over Hospital expansion courtesy of wikimedia commons.
How to Reduce  Plaque : Track Your Plaque
Plaque : Track Your Plaque
Atheroscleorosis
is a bad thing. How do we prevent it ? How do we halt progression of
all these atherosclerotic plaques in our arteries? Should we use drugs,
diet or lifestyle modifications ? This is where the "Track Your Plaque
Program " comes in, devoted to halting progression of plaque formation
with diet and lifestyle changes.
Rather than re-invent the wheel, we have adopted the William Davis MD program called
"Track Your Plaque".
With this program we can estimate heart attack risk by measuring plaque
size and growth with serial calcium scores. The program also uses the
advanced lipoprotein profile as another way to monitor response to diet
and lifestyle modification. This is all discussed in
part one.
A Differing Viewpoint - The Plumbers Are Wrong
Dr. Thomas Cowan in the May 2014 Townsend Letter
begs to differ and proposes an alternate theory called the
Myogenic Theory. A .pdf of the May 2014 article can be read by clicking here:
Thomas_Cowan_What_Causes_Heart_Attacks.
Although arterial plaque is a bad thing, Dr Cowan
says the Plumbing approach to clogged arteries is all wrong, and for the most part a futile exercise.
Left image: Diagram showing Coronary Stenting Procedure Courtesy of NIH and Wikimedia Commons.
 Left image: Diagram showing Coronary Stenting Procedure Courtesy of NIH and
Left image: Diagram showing Coronary Stenting Procedure Courtesy of NIH and
In
agreement with Dr. Cowan is Howard H. Wayne, M.D. who lists 39 studies
published in the mainstream cardiology literature proving the futility
of the Plumbing approach.
Dr. Wayne
says (quote)
"almost
every single study....clearly and unequivocally demonstrates that
invasive treatment, be it bypass surgery or angioplasty, fail to reduce heart attacks and mortality when compared to patients who have been conservatively treated with medication. In addition, there is a clear increase in mortality....in the invasively treated patients. (End Quote Dr Wayne)
Of course, the favorite study quoted is the large
2003 Mayo Clinic study
which concludes that bypass relieves chest pain but does not prevent
further heart attacks, and that those who benefit from bypass surgery
are the high risk patients whose lives are in acute danger.
Problems with the Plumbing Approach
The
"plumbing approach" to coronary artery disease with stents and bypass
operations has been a disappointment with no reduction in mortality
compared to medical treatment for the patient with chronic stable
angina. However, there is a plumbing benefit, as mentioned above, for
the high risk patient. We will now look into this to find out why.
With
the exception of the bypass or stent for the "high risk patient" such
as the left main coronary artery lesion, also known as the
"Widow Maker",
cardiac "plumbing" procedures have been a disappointment. In the
stable angina patient, benefits of plumbing procedures are about the
same as medical treatment. Why is that?
Formation of Collateral Circulation
 A Quick Trip to the Dog Lab
A Quick Trip to the Dog Lab
A 1976
study from
the dog lab is illustrative. When the dog's coronary artery is
suddenly occluded, the dog suffers a heart attack and could die.
However, if the dog's coronary artery is gradually occluded over four
days, the dog's heart develops extensive collateral vessels which
prevent myocardial infarction. The collateral vessels have done their
job. This dog has a completed occluded coronary artery with no heart
attack nor cardiac damage.
Quote from study:
"When the time to
complete occlusion was 4 days, myocardial infarction was prevented due
to growth-transformation of pre-existing collaterals." Quote from Dr. Schaper Circ 1976.
The formation of well developed collaterals has "
survival benefit"
protects us from heart attacks, serving as our own personal bypass
operation courtesy of mother nature. This explains the value of medical
treatment with Beta-Blockers and other cardiac drugs which buy time for
our heart to develop collateral circulation.
EECP
Formation
of collateral vesels is one of the expected outcomes of a procedure
called EECP EKG-Gated Extracorporal Counter Pulsation. My previous
article on EECP discussed this.
Autonomic Nervous System- Parasympathetic vs Sympathetic
Dr. Cowan tells us something we already know. The heart is very sensitive to our emotional state. Our language is filled with
idioms
and phases relating to the heart, such as "She broke my heart".. People
have been known to succumb from heart attack on the basis of a sudden
severe emotional shock, fear, grief etc. This is called the
Broken Heart Syndrome as described by Dr. Wittstein in the
Cleveland Clinic Journal of Medicine(2007).
Our
physiology colleagues have studied the nervous innervation to the heart. Luckily for us, the heart beat is automatic, controlled by the
autonomic nervous system consisting of the sympathetic branch which speeds up the heart rate, and the
parasympathetic branch (from the Vagus Nerve) which slows down the heart rate.
Studies of the autonomic nervous system using
heart rate variability monitors show that patients with reduced parasympathetic activity have
higher risk for heart attack, and that heart attack victims have
reduced parasympathetic activity.
Dr.
Sroka, an expert on the autonomic nervous system, reports that heart
attack victims will show a peculiar sudden drop-off of parasympathetic
activity just prior to their heart attack. In addition, this reduction
in parasympathetic activity can be prevented by Ouabain, an endogenous
cardiac steroid which restores parasympathetic activity by enhancing
release of its principal neurotransmitter ACH (Acetlycholine) .
Read
the .pdf of Dr Sroka's article on Myocardial Ischemia in which he
proposes that ischemic events can be triggered by the autonomic nervous
system. This could certainly explain the reported cases of heart
attacks with completely normal coronary arteries:
Sroka_Myocardial_Ischemia_ANS
 Medical Armamentarium
Medical Armamentarium
Beta Blockers, Calcium Chanel Blockers, Nitrates, Aspirin and other blood thinners are
typically used for medical treatment of the stable angina patient.
Above left chemcial structure of Ouabain, Notice steroidal ring component. courtesy of Wikimedia commons.
Enter the Cardiac Glycoside- Ouabain
Dr,
Thomas Cowen again differs from mainstream cardiology in his drug of
choice for medical treatment of the stable angina patient. Dr. Cowan
reports great success with an old botanical drug called Ouabain, also
called
Strophanthus (Strodival),
obtained from an African plant, and still in use by cardiologists in
Germany obtainable from local German pharmacies. Dr Cowan reports that
in his office practice this medication has been successful in
preventing heart attacks.
 The Endogenous Cardiac Glycosides
The Endogenous Cardiac Glycosides
In 1991 researchers discovered that Ouabain from the Strophanthus plant is identical to our own
endogenous cardiac glycosides made by the adrenal gland. Digoxin (Digitalis from the Foxglove plant) is another one of the endogenous cardiac glycosides.
Above image shows chemical structure of endogenous cardiac steroids courtesy of Schoner 2007.
Benefits in Cardiac Ischemia, Angina, and Infarction
Both animal (
Vatner) and human studies (
Sharma)
show striking benefits to the myocardium during ischemic events by
using an ouabain preparation called Strodival/Strophanthum.(5-18).
Indeed, Ouabain has been dubbed "the insulin of the heart": Click Here
to read pdf article:
Ouabain_the_insulin_of_the_heart.
More on Ouabain/Strophanthun clinical experience from Dr Debusman, a German cardiologist.
More on Ouabain by Dr. Sroka.
Conclusion:
The story is familiar. A natural plant botanical substance, Ouabain,
sharing its identity with an endogenous hormone produced by the adrenal
gland, exhibits striking health benefits for angina, ischemia, and
myocardial infarction prevention. Yet this natural drug is largely
ignored by mainstream cardiology because it cannot be patented, and
therefore lacking in large controlled studies.
Link To Online Store for Tea Brasil TIncture of Ouabain.
Strophantin
Mother tincture , Ouabain, Quabain, (Strophantus gratus) 120ml.
strophantin, Strophanthin, Strophantus gratus, strophantus gratus,
strodival, kombetin, Ouabain, Acocantherin, Astrobain, G-Strophicor,
Gratibain, Gratus, Strophanthin, Kombetin, Purostrophan, Rectobaina,
Solufantina, Strodival, Strophalen, Strophoperm, Strophosan, Uabaina,
Uabanin, Estrofantina
120 ml USD 69,00
Articles with Related Interest:'
Preventing Heart Disease
Parts one,
two,
three and
four
Jeffrey Dach MD
7450 Griffin Road Suite 190
Davie, Florida 33314
954-792-4663
Links and References:
Endogenous Cardiac Glycosidess
1)
Endogenous_exogenous_cardiac_glycosides
2)
Endogenous_Cardiac_Glycosides
3)
http://www.townsendletter.com/May2014/May2014.html
What Causes Heart Attacks by Dr. Thomas Cowan
The conventional view of the cause of heart disease is that the central
events occur in the coronary arteries. Dr. Cowan rebuts this theory,
laying out the case that heart disease is actually better understood
from the perspective of events happening in the myocardium, and
describing the precise and well-documented events that do lead to heart
attacks.
Also see:
http://www.westonaprice.org/modern-diseases/what-causes-heart-attacks/
4)
http://fourfoldhealing.com/2010/06/08/what-causes-heart-attacks/
What Causes Heart Attacks Posted on June 8, 2010 by Thomas Cowan, M.D.
In my practice, I generally use oral strophanthin in the form of the
preparation known as Strodival for all my angina and MI patients, and I
have uniformly recorded a decrease in angina episodes, improved exercise
tolerance and, thus far, no MIs. When combined with a nourishing
traditional diet, cod liver oil, high vitamin butter oil, CoQ10 (which
helps strengthen the heart muscle) and Standard Process heart nutrients
(Cardioplus, two capsules three times per day, and Cataplex E2, two
tablets three times per day),
5)
http://www.melhorn.de/Strophhormon2/
Cardiac Infarction g-Strophanthin ( Ouabain ) - the Endogenous Hormone. Dr. rer.nat.Rainer Moser Diploma chemist
6)
http://www.wrf.org/alternative-therapies/g-strophantin-heart-disease.php
Rolf-Jurgen Petry January 25, 2009
Strophanthin
/ ouabain is free available in German pharmacies as a homeopathic
medicine ("Strophactiv" from the company "magnetactiv"). D4 = 1:10.000,
there is enough substance in it to generate a substantial effect,
additionally to the homeopathic effect.
Allopathic / substantial
ouabain ("Strodival") is available only with a prescription from a
physician. You can get it at the pharmacy of the Airport of Munich,
likely also at other German airports or international pharmacies.
Strodival
mr = enteric-coated capsules with 3 mg each for prophylaxis. Strodival =
capsules to bite (adsorption with the tongue and mouth) with 3 mg each
for acute situations.
Strodival spezial with 6 mg is not available any more.
The
pharmacy "Schloss-Apotheke" in Koblenz / Germany makes a ouabain
solution, and also ouabain pharmaceutical phials for intravenous
injection, likely they sell it abroad with a prescription. Tel.
0049-261-18439
More information about ouabain on
http://ouabain.twoday.net
Best
wishes, Rolf-Jurgen Petry (author of a book about ouabain with 1665
references and a preface from Prof. Hans Schaefer (Heidelberg), who was a
world-famous physiolgist for decades (available only in German language
yet, is there an edition who wants to translate it into English ?)
Strodival Info
September 12, 2009
International Reseller of Strodival:
Masters Pharmaceuticals Ltd
Unit 380, Centennial Avenue
Centennial Park, Elstree
Hertfordshire WD6 3TJ
UK
Tel: 0208 327 0900
Fax: 0208 327 0901
---------------------
US TOLL FREE Tel: 1-800-969-1152 FAX: 1-800-969-1153
7)
http://www.strophantus.de/printversion.html
Dr Debusmann What is Strophanthin?
Dr. Wieland Debusmann who had a heart attack himself at the young age
of 42, is the expert on ouabain. On his detailed website –
www.strophantus.de
– all aspects of ouabain are dealt with in English. Rolf-Jürgen Petry
has written a very good book “Strophanthin” (89). His website –
www.strophanthin.org – is also instructive and available in English.
Strophanthin
was, by chance, discovered in Africa in 1859. In England processed, in
France analysed and in Germany first used with great
health-effective-qualities, by Prof. Albert Fraenkel (v. interesting
piece in wikipedia) intravenously. Fraenkels boss was Prof. Ludolf von
Krehl. Both founded important clinics in Heidelberg and Badenweiler and
well-known medical prizes are named after them.
When in 1924 Prof.
Ernst Edens (3), Ordinarius of Medicin University Clinic Düsseldorf
presented to his intern colleagues his outstanding experiences with
Strophanthin as a cure for Angina pectoris and Heart attacks he earned,
curiously, not just euphoria but also scepticism and rejection.
Prof
Ernst Edens (3) said, “not using Strophanthin is a medical mistake”.
Until about 1975 Strophanthin was used intravenously with success in
nearly all hospitals and university clinics in Germany and is until
today, known for its good effect by all older doctors. Also, older
experienced nurses have confirmed to me the great reputation of
Strophanthin. Also the oral preparate (orally and not intravenously)
developed since 1947, displays convincing results. Even though today it
is nearly the best and side-effect free heart remedy, the opinion of the
medical academics is:
a. it doesn’t work
b. it is highly poisonous
c. there are better remedies today
In response to a:
98 % of all doctors that have used or continued to use it, have
observed an extremely high effectiveness, the other 2 % remain within
limits, positive. None of the doctors asked were negative about its
effectiveness. (Questionnaire from 3650 doctors, 1984) (4).
A
placebo controlled, double blind study observed a highly significant
effectiveness of orally taken Strophanthin. All Angina pectoris patients
experienced an improved EKG and well-feeling, the most a marked
improvement in condition (5).
Prof. Dormann used Strophanthin
capsules for 12 years in a large Berlin hospital: 99 % of patients with
Angina pectoris took a stomach acid resistant capsule and were complaint
free after 2 weeks (82 % after 1 week), all previous remedies were
omitted (6).
8)
http://heartattacknew.com/faq/what-can-be-done-to-prevent-a-heart-attack/ouabain-the-wasted-opportunity/
Ouabain the wasted opportunity
9)
http://heartattacknew.com/
strophanthin Knut Sroka, MD
10)
http://www.infarctcombat.org/
Fighting Heart Disease through Information, Research and Education.
Carlos E. T. B. Monteiro is an independent researcher and scientist from
Brazil having an experience of about 43 years in dealing with medical
matters.
In 1972 he turned to be a disciple and follower in the
scientific plan from Dr. Quintiliano H. de Mesquita, who has developed
the myogenic theory of myocardial infarction and other pioneer
contributions to medical literature (QHM Memorial). Carlos Monteiro has
accompanied Dr. Mesquita as a special collaborator until his death in
2000.
In 1999 he participated in the foundation of Infarct Combat
Project and elected president by the board of directors with the support
from Dr. Mesquita who was one of the members.
Carlos Monteiro
still defending Dr. Mesquita’s medical and scientific ideas, through
Infarct Combat Project. Recently he has developed a new hypothesis to
explain atherosclerosis that was named acidity theory of
atherosclerosis. The blog new evidences about his Acidity Theory you can
find here http://www.infarctcombat.org/MyogenicTheory.html
================================================
11)
Coronary_Arteries_Acute_Myocardial_Infarction_Circulation_Roberts_1972
Roberts, William C. "Coronary arteries in fatal acute myocardial infarction." Circulation 45.1 (1972): 215-230.
-----------------------
12)
http://www.ncbi.nlm.nih.gov/pubmed/9781964
Am
J Cardiol. 1998 Oct 1;82(7):839-44.Intracoronary aspiration
thrombectomy for acute myocardial infarction. Murakami T1, Mizuno S,
Takahashi Y, Ohsato K, Moriuchi I, Arai Y, Mifune J, Shimizu M, Ohnaka
M.Department of Cardiology, Fukui Cardiovascular Center, Shimbo, Japan.
To
investigate the pathogenesis of acute myocardial infarction (AMI) and
values of intracoronary aspiration thrombectomy (ICAT), we applied ICAT
to reperfusion therapy using generally available intracoronary catheters
to aspirate intracoronary occlusive tissues. We assigned ICAT or
primary percutaneous transluminal coronary angioplasty (PTCA) to
patients with evolving AMI (Thrombolysis In Myocardial Infarction (TIMI)
trial grade 0), and investigated primary histopathologic, clinical, and
angiographic outcomes in 43 patients treated with ICAT alone or
followed by PTCA, and compared the outcomes with those in 48 patients
treated with primary PTCA. No major complications (procedural death,
emergent bypass graft surgery) occurred. Reconalization (TIMI grade 3
and 2) was achieved in 25 patients (58%) with ICAT alone and in 39
patients (91%) with ICAT alone or followed by PTCA. Aspirated thrombi
were defined as recent thrombi in 21 cases (49%), atheroma in 6 (14%),
no thrombi in 13 (30%), and organized thrombi in 1 case. In cases of
recent thrombi, ICAT alone provided recanalization more frequently than
in those of atheroma or no thrombi (18 of 21 [86%], 3 of 6 [50%], 4 of
13 [31%], respectively; p < 0.05; recent thrombi vs atheroma or no
thrombi). There were no significant differences in primary
recanalization rate (ICAT alone or followed by PTCA vs primary PTCA; 91%
vs 92%) or incidence of complications between the 2 strategies. These
results indicate that although the pathogenesis of AMI is heterogeneous
in each individual case, intracoronary thrombus contributes little to
the pathogenesis of average AMI, and therefore mechanical approaches may
be feasible to maximize reperfusion therapies for AMI.
13)
http://www.ncbi.nlm.nih.gov/pubmed/9781974
Am J Cardiol. 1998 Oct 1;82(7):896-7.
Coronary thrombosis during acute myocardial infarction: Roberts was
right! O'Neill WW.Pathologic studies have varied with clinical belief
regarding the role of acute thrombotic occlusion as the inciting event
during myocardial infarction. Aspiration thrombectomy, by employing a
new catheter, has been performed during myocardial infarction and
confirms the pathologic findings that intracoronary thrombus is absent
in a substantial number of patients with acute myocardial infarction.
Roberts, William C. "Coronary arteries in fatal acute myocardial infarction." Circulation 45.1 (1972): 215-230.
Spain,
David M., and Victoria A. Bradess. "The Relationship of Coronary
Thrombosis to Coronary Atherosclerosis and Ischemic Heart Disease:(A
Necropsy Study Covering A Period of 25 Years)." The American Journal of
the Medical Sciences 240.6 (1960): 69-78.
Frequency of
coronary thrombosis related to duration of survival from onset of acute
fatal episodes of myocardial ischemia. Circulation, 22:816, 1960)
Spain,
D. M., and Victoria A. Bradess. "Frequency of coronary thrombi as
related to duration of survival from onset of acute fatal episodes of
myocardial ischemia." Circulation. Vol. 22. No. 4. 227 EAST WASHINGTON
SQ, PHILADELPHIA, PA 19106: LIPPINCOTT WILLIAMS & WILKINS, 1960.
"The
coronary patient does not die from coronary disease, he dies from
myocardial disease.“**Burch GE and col., Ischemic cardiomyopathy, Am
Heart J. 1972
Mar;83(3):340-50++++++++++++++===============================================================
Thomas Cowan Web Site on Heart Disease
16)
http://heartattacknew.com/
Knut Sroka MD
Fig. 1: Defect in the “PNS” expressed by an almost “rigid pulse rate” PNS= Parasympathetic Nervous System
This
simple illustration provides surprising information. The upper curve is
that of a healthy person, the lower that of a person with coronary
heart disease. The upper curve shows a typically normal wave-like
pattern during 6 deep breaths. The lower curve shows an almost ”rigid
pulse” (33). The above graph is a very good example of the defective PNS
function in a heart patient.
Based on my own research and on a
dozen international studies, the relationship between PNS reduction and
heart seizure is presented in my comprehensive article “On the genesis
of myocardial ischemia” (17). According to these studies, about ¾ of all
heart seizures are triggered in this way.
Uninhibited SNS
impulses on the heart, when the PNS brake is blocked, present a
constellation, which results in heart seizure and heart attack (17).
A
bloodless (“ischemic”) area then develops. Please note that such a
bloodless area does not arise as a result of circulation problems due to
blocked coronary arteries. This bloodless area is the result of an
acute overexpansion of parts of the heart muscle, ultimately the result
of a defect in PNS heart control.
Chronic stable angina: In 2003, a
very good publication from the Mayo Clinic (1), USA, which I have
already quoted on the subject of “bypass surgery” (Section 1) stated the
following:
Balloon and stents are suitable for reducing complaints, i.e. for relieving symptoms.
Balloons and stents do not prevent heart attacks and do not prolong life.
Stents prevent the development of renewed stenoses at the same location
in the vessel, but do not reduce the frequency of heart attacks or
deaths.
Ouabain increases the heart’s performance, without
increasing the oxygen consumption (77). And very important: when the
heart metabolism is whipped up by adrenaline, then ouabain reduces the
oxygen consumption of the heart (78). In such a situation, as is the
case during a heart seizure, ouabain has an oxygen-saving effect.
German
pharmacologist of the time, H. Gremels, had, as early as the 1930’s,
clearly shown that ouabain drastically increases the effects of the PNS
on the heart within a few minutes (up to a maximum of 1000 times
greater). The effect of the SNS is reduced; and even the smallest doses
of ouabain have the full effect (78).
Dr. Wieland Debusmann, who
had a heart attack himself at the young age of 42, is an expert on
ouabain. On his detailed website –
www.strophantus.de –
http://www.strophantus.de/in-english-1.html
((((((((((((((((((( ++++++++++++++ !!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
17)
ouabain_the_insulin_of_the_heart full pdf
PERSPECTIVE CUNICAL PRACTICE - Ouabain - the insulin of the heart. lnt J Clin Pract, November 2010, 64, 12, 1591-1594
This
effect was the basis for the chance discovery of ouabain in 1859 by be
English botanist Kirk. He bad discovered the fast onset of action of
ouabain on the heart by using a
toothbrusb contaminated witb Strophanthus seeds.
The
rapid onset of effect of oral ouabain was used in medical practice for a
'Strophanthin-quick-test': patients with suspected heart disease were
given two tablets of 3 mg that they had to chew and distribute in the
mouth. In the case of heart disease, a relief of complaints was observed
within 5-10 min. This test was used routinely in German physicians'
offices well as into the 1970s.
Strodival®rnr
by Medapharrna (Meda Pharrna GmbH & Co. KG, Bad Hornburg v.d.H., Gerrnany).
18)
http://ouabain.twoday.net/
Strodival mr® (3 mg) from MEDA, Bad Homburg/Germany
The dosage is declared as 1 - 4 x 3 - 6 mg daily; principally success
and demand should regulate the dosage. There is no real danger of
overdosage as often seen with digitalis preparations.
19)
http://www.ajconline.org/article/0002-9149%2865%2990704-6/abstract
American Journal of Cardiology
Volume 16, Issue 6 , Pages 859-880, December 1965
Acute coronary occlusion as a cause of myocardial infarct and sudden coronary heart death
Giorgio Baroldi, M.D.
The
incidence of acute occlusion was investigated in 208 hospitalized
patients dying from acute or recent coagulative necrosis of the
myocardium, in 116 cases of sudden, unexpected “coronary” heart death,
and in 125 cases of sudden but not unexpected “coronary” heart death.
The approximate ages of both the vascular and myocardial lesions and the
prior sclerotic reduction of the lumen of the acute or recently
occluded vessels were studied and correlated with the corresponding
enlargement of the collateral arterial circulation.
From the high
incidence of acute or recent coagulation necrosis and/or sudden heart
death without acute occlusion (53, 53, and 54% in the three groups
studied), the low incidence of a “coeval” relation between the acute or
recent occlusion and the stage of the myocardial damage (23, 22, and
19%, respectively), the high incidence of sclerotic reduction of the
lumen in excess of 65 per cent in the acutely or recently occluded
vessels (82, 91, and 96%, respectively), and the marked enlargement of
the collateral circulation found in this study, it appears that in the
so-called myocardial infarct or the sudden “coronary” heart death in the
human being, most of the cases develop independently of an acute
occlusion and that it is incorrect to apply the term “myocardial
infarct” to the lesions. It is also our belief that the acute or recent
thrombosis occurring in most of the instances should not be considered
as the cause of the acute or recent myocardial coagulative necrosis or
sudden death or both, but rather as the result of particular hemodynamic
conditions existing in and around the involved vessel.
21) full pdf
Coronary Thrombosis and Fatal Myocardial Ischemia
WILLIAM C. ROBERTS Circulation. 1974;49:1-3
In
conclusion, there is substantial evidence that acute thrombus formation
does not precipitate acute fatal IHD. The major problem is diffuse
generalized coronary atherosclerosis with severe (>75%) luminal narrowing (at least 2 of the 3 major coronary arteries).
full pdf
22)
Silver, MALCOLM D., GIORGIo Baroldi, and F. A. B. I. O. Mariani. "
The relationship between acute occlusive coronary thrombi and myocardial
infarction studied in 100 consecutive patients."
Circulation 61.2 (1980): 219-227.
These data support the concept that an occlusive coronary thrombus has no
primary role in the pathogenesis of a myocardial infarct.
These data support the concept that an occlusive coronary thrombus has no
primary role in the pathogenesis of a myocardial infarct.
SUMMARY A prospective study was done on 100 hearts from patients who had clinically proved myocardial
infarction with histologic confirmation. The following variables were
considered and related statistically: age, set and duration of patient
survival; heart weight; type, form, length and degree of preexisting
stenosis in the coronary system; the location and type of coronary
occlusion; the location, type and size of an infarct and the other forms
of irreversible myocardial damage found. Fifty-five percent of the
hearts had no occlusive thrombus in the coronary artery supplying the
infarcted myocardium. In 45 cases in which thrombi were found, all but
one were in a supplying coronary artery. The occurrence of thrombi was
associated with an increased size of infarct, most frequently with
transmural infarcts (55%) and less often with those involving the inner
two thirds of the wall (30%) or with subendocardial infarcts (27%). Most
infarcts developed in patients with 70% stenosis in the coronary
artery system, although the size of an infarct was independent of the
number, degree, length and distribution of severe stenoses found in the
system. A supplying artery usually showed a stenosis of > 70% along
its course or, if it contained an acute occlusive thrombus, the thrombus
was at a stenosis caused by an atheromatous plaque. These data support
the concept that an occlusive coronary thrombus has no primary role in
the pathogenesis of a myocardial infarct.
23)
http://www.ncbi.nlm.nih.gov/pubmed/8033829
Endocrinology. 1994 Aug;135(2):794-7.
Ouabain is secreted by bovine adrenocortical cells.
Laredo J1, Hamilton BP, Hamlyn JM. 1Department of Physiology, University of Maryland, Baltimore 21201.
Ouabain is a specific inhibitor of the sodium pump. This steroid has
been found in the mammalian circulation in significant amounts and may
be of adrenal origin. Secretion of ouabain from adrenal cells has been
little studied and the purpose of the present work was to determine the
adrenal distribution of ouabain, aldosterone and cortisol, and to
characterize the effects of ACTH and angiotensin II on the secretion of
these steroids in primary cultures of bovine adrenocortical cells. In
fresh bovine adrenals, the cortical to medullary ratios for aldosterone,
cortisol and ouabain were 14, 4.25 and 2.5, respectively. All three
steroids were detected in elevated amounts in the conditioned medium of
primary cultures of adrenocortical cells. Reverse phase HPLC of the
secreted ouabain immunoreactivity showed it was isopolar with commercial
ouabain. In the presence of 10 nM ACTH or angiotensin II, the secretion
of all three steroids increased significantly with similar time
courses. The stimulated secretion of ouabain exceeded the intracellular
content of this steroid in either control or activated cells by 3-5
fold. The amount of angiotensin II stimulated ouabain secretion was
greater from cells incubated in larger volumes. These results show that
ouabain is enriched in the bovine adrenal cortex, and is secreted by
primary cultures of these cells. The secretion of ouabain is increased
by ACTH and angiotensin II, is due to either de novo synthesis or
transformation of an intracellular precursor that is not overtly
immunoreactive, and is feedback regulated by either ouabain itself or a
cosecreted factor. These cells may be useful to study stimulus-secretion
coupling and the biosynthetic pathway of ouabain.
24)
http://www.ncbi.nlm.nih.gov/pubmed/8593799
Endocrinology. 1996 Feb;137(2):533-9.
Ouabain production by cultured adrenal cells.
Doris PA1, Hayward-Lester A, Bourne D, Stocco DM.
The adrenal cortex releases a sodium pump inhibitor. The present
studies tested whether this material was endogenous and identical to
ouabain by 1) studying the production of ouabain in long term cultures
of adrenocortical cells, 2) seeking evidence that ouabain might be taken
up from exogenous sources by adrenocortical cells, 3) examining the
release of adrenocortical cells loaded with exogenous ouabain, 4)
attempting to stimulate ouabain steroidogenesis in cultured
adrenocortical cells, and 5) performing further chemical analysis on
ouabain immunoreactivity released by cultured adrenocortical cells. Our
results indicate that ouabain immunoreactivity is present in conditioned
medium from both murine Y-1 adrenocortical cultures and primary bovine
adrenocortical cell (BAC) cultures. We also found that BACs bind and
internalize [3H]ouabain. Bound [3H]ouabain is released from BACs by both
receptor dissociation and cytoplasmic release of internalized
[3H]ouabain. Only one isoform of membrane sodium, potassium-adenosine
triphosphatase, alpha 1, was expressed in the adrenal. Authentic ouabain
was not metabolized during membrane binding or while present
intracellularly. Stimulation of steroidogenesis in Y-1 and BAC with
22R-hydroxycholesterol and 25-hydroxycholesterol was performed and
confirmed increased steroidogenesis; however, there was no effect on
ouabain immunoreactivity content or release. Comparison of the ouabain
binding density in cultured BAC, hepatoma cells, and 3T3 fibroblasts
indicated that adrenocortical cells have a high ouabain-binding
capacity. HPLC studies of the ouabain immunoreactivity released by
bovine adrenocortical cells indicated that essentially no authentic
ouabain was secreted. The present studies confirm that both BAC and Y-1
cultures release a ouabain-like material that differs in structure from
authentic plant ouabain and is not a product of cholesterol side-chain
cleavage.
25)
http://www.ncbi.nlm.nih.gov/pubmed/9792206
Gen Pharmacol. 1998 Oct;31(4):499-501.
Is ouabain produced by the adrenal gland?
Foster RH1, Prat H, Rothman I.
1. Ouabain or a related stereoisomer, termed endogenous ouabain, has
been identified in adrenal cortex tissue and culture medium from
adrenocortical cells. 2. Angiotensin II and adrenocorticotropin, the
main activators of aldosterone secretion from adrenal glomerulosa cells
appear to increase the production of this compound. 3. The purpose of
this review is to briefly discuss recent available experimental evidence
suggesting that endogenous ouabain is secreted by the zona glomerulosa
of the adrenal gland.
==============================
==============================
==============================
========
26)
http://circ.ahajournals.org/content/49/6/1127.short
Necropsy Studies in Myocardial Infarction with Minimal or No Coronary
Luminal Reduction Due to Atherosclerosis R. S. ELIOT, M.D.; G.
BAROLDI, M.D.; A. LEONE, M.D.+ Author Affiliations From the
University of Nebraska, Division of Cardiology, Department of Medicine,
the Institute of Morbid Anatomy, School of Medicine, University of Milan
and CNR Institute Fisiologic Clinica, Medical School, University of
Pisa, Italy.
A postmortem study was conducted on the hearts of 10
patients who died with a typical clinical picture of acute myocardial
infarction within 25 days of onset of symptoms. The coronary arterial
systems of the patients revealed minimal or no luminal reduction due to
coronary atherosclerosis or other cause. These cases contribute to the
understanding of the pathogenesis of acute myocardial infarction in that
they document the presence of typical acute myocardial infarction in
the absence of chronic or acute coronary arterial obstruction. They
further suggest that the hearts of those dying of typical myocardial
infarction show minimal or no coronary disease in approximately 7% when
studied as described.
http://www.ncbi.nlm.nih.gov/pubmed/837499
Circulation. 1977 Apr;55(4):578-80.
The nature and clinical features of myocardial infarction with normal coronary arteriogram.
Rosenblatt A, Selzer A.
Abstract
Six
new cases of acute myocardial infarction with normal coronary
arteriogram are presented and supplemented by 19 collected cases (group
I). These are compared with 16 cases of myocardial infarction caused by
occlusive coronary artery disease in a comparable population (group ii).
The following significant differences between the two groups are
established: patients in group I were younger (27.5 years vs 33.7 years,
P less than 0.005); at least one risk factor was present in all
patients in group II, but in only 40% of group I (P less than 0.0001).
effort angina preceded the attack in ten patients of group II, but in
none of group I (P less than 0.0001). The attack was unheralded in 24 of
the 25 patients in group I, but was preceded by prodromes in 11 of 16
in group II (P less than 0.0001). Attacks of pain following myocardial
infarction occurred in five patients of group 2 and II of group II) (P
less than 0.001). Results are discussed in the light of the nature of
myocardial infarction in group I. No support is found for the coronary
spasm theory. The most likely mechanism for development of myocardial
infarction in group I is thought to be a thromboembolic "accident." This
accident is not necessarily related to atherosclerotic coronary disease
and is presumed to be benign in nature.
http://www.ncbi.nlm.nih.gov/pubmed/7246444
Am J Cardiol. 1981 Jul;48(1):28-32.
Myocardial infarction with normal coronary arteries: a prospective clinical-angiographic study.
Betriu A, Pare JC, Sanz GA, Casals F, Magriña J, Castañer A, Navarro-Lopez F.
Abstract
The
association of myocardial infarction with normal coronary arteries was
analyzed prospectively. A series of 259 consecutive men aged 60 years or
less underwent selective coronary angiography 30 days after a definite
infarct. Coronary arterial lesions were documented in 251 patients,
normal coronary arteries in the remaining 8. The latter patients had a
significantly lower (p less than 0.001) mean age than the former; no
patient older than 50 years had patent coronary arteries, whereas 5 of
the 11 patients under age 35 had normal arteries. The prevalence of risk
factors was similar in both groups of patients. Although there were no
group differences in infarct size or location, patients with normal
coronary arteries had a higher ejection fraction (p less than 0.01) and a
lower left ventricular end-diastolic pressure (p less than 0.05). A
previous history of angina or infarction and the occurrence of new
coronary events were confined to patients with coronary arterial
lesions. The clinical course of patients presenting with normal
angiograms was uneventful. Transient coronary occlusion, the most likely
mechanism of infarction in this group of patients, could not be
ascribed to either spasm or platelet hyperactivity.
http://www.ncbi.nlm.nih.gov/pubmed/15227036
Tex Heart Inst J. 1985 Mar;12(1):1-7.
Acute myocardial infarction with "normal" coronary arteries: clinical
and angiographic profiles, with ergonovine testing. Salem BI1, Haikal
M, Zambrano A, Bollis A, Gowda S.
Author information 1Cardiac
Catheterization Laboratory, 224 South Wood Mill Road, Suite 710,
Chesterfield, Missouri 63017, USA.
Abstract Among 528 patients
consecutively undergoing selective coronary angiography after acute
myocardial infarction, ten cases (1.9%) with angiographically normal
coronary arteries were identified. Eight of these ten patients were 45
years of age or younger and comprised 11% of those studied in this age
group, with higher prevalence in females (five of 18 [28%]) versus
males, (three of 57 [5%]). Common features besides the young age of
patients included predominance of female sex, smoking as a risk factor,
and the lack of preinfarction symptoms. An ergonovine test was carried
out in seven of these patients, and all tested patients failed to show
any evidence of focal coronary spasm. Three patients had recanalization
of the infarct-related vessel by intracoronary streptokinase. The lack
of a history of variant angina in nine patients, the negative response
to ergonovine provocation in seven, and documented thrombolysis after
intracoronary streptokinase in three seem to indicate that a thrombotic
process is a leading factor in myocardial infarction in such cases.
Angiographic studies of this young subset of patients would enhance
their identification and might reveal the pathophysiologic mechanisms
involved with potentially significant clinical implications. Long-term
follow-up of such cases will be needed to determine their ultimate
prognosis.
http://www.ncbi.nlm.nih.gov/pubmed/11482919
Eur Heart J. 2001 Aug;22(16):1459-65.
Clinical characteristics, aetiological factors and long-term prognosis
of myocardial infarction with an absolutely normal coronary angiogram; a
3-year follow-up study of 91 patients.
Da Costa A1, Isaaz K, Faure E, Mourot S, Cerisier A, Lamaud M.
The
purpose of this study was to evaluate the clinical outcome of a large
cohort of patients who suffered an acute myocardial infarction with
absolutely normal epicardial coronary arteries at the post-myocardial
infarction coronary angiogram. The aetiological and prognostic factors
in this population were also analysed.
BACKGROUND:Few data exist
concerning the outcome, and aetiological and prognostic factors, of
patients with myocardial infarction and angiographically absolutely
normal coronary arteries.
METHODS:Ninety-one patients (34 females/57
males; mean age 50+/-13 years, range 24--78 years) admitted with an
acute myocardial infarction had absolutely normal coronary arteries at
the angiogram performed 6.2+/-4 days (range 1--15 days) after the
myocardial infarction, defined by smooth contours and no focal reduction
(NC). Of the 91 NC patients, 71 were evaluated prospectively, alongside
a systematic search of all aetiological factors reported in the
literature. The NC patients were matched for age, sex, and the same
period of myocardial infarction onset with a group of 91 patients with
coronary artery stenosis (>50% diameter stenosis) at the angiogram
performed 7.3+/-4 days (range 1--15 days) after the myocardial
infarction (SC).
RESULTS:The percent of smokers was similar between
the two groups; higher prevalence rates of coronary heart disease family
history, obesity, hypertension, hypercholesterolaemia and diabetes
mellitus were found in SC (P=0.043 to 0.0001). In NC, coronary spasm was
found in 15.5%, congenital coagulation disorders in 12.8%, collagen
tissue disorders in 2.2%, embolization in 2.2%, and oral contraceptive
use in 1.1%. Left ventricular ejection fraction at hospital discharge
was higher in NC (60%+/-13%) than in SC (55%+/-13%, P=0.04). The mean
follow-up was 35 months (range 1--100 months). Kaplan-Meier event-free
survival, with the combined end-point defined as death, reinfarction,
heart failure and stroke was 75% in NC vs 50% in SC (P<0.0001).
Survival rate was 94.5% in NC compared to 92% in SC (ns). Univariate
predictors of events in NC were left ventricular ejection fraction
(P=0.03), age (P=0.02), diabetes (P=0.01), and smoking (P=0.03). Using
Cox multivariate analysis, independent predictors of long-term outcome
in NC patients were left ventricular ejection fraction (P=0.003) and
diabetes (P=0.004).
CONCLUSION:Aetiological factors, predominantly
coronary spasm and inherited coagulation disorder, can be detected in
only one third of the patients with myocardial infarction and absolutely
normal coronary angiograms despite a systematic search in a prospective
population. Mortality rates are similar but morbidity is lower in
myocardial infarction patients with absolutely normal coronary
angiography compared with those with coronary artery stenosis. The only
two independent factors predictive of poor outcome in myocardial
infarction patients with normal coronary arteries are left ventricular
function and diabetes.
http://www.ncbi.nlm.nih.gov/pubmed/506362
Z Kardiol. 1979 Aug;68(8):534-40.
[Coronary reserve, left ventricular function, and coronary risk factors
in patients with myocardial infarction, but normal coronary arteries
(author's transl)].
[Article in German] Opherk D, Mäurer W, Mehmel HC, Müller JH, Zebe H, Kübler W.
Abstract In 5 patients with angiographically normal coronary arteries
and previous myocardial infarction (left ventricular a- or dyscinesia),
measurement of coronary reserve revealed normal values. On average,
patients with myocardial infarction and normal coronary arteries were
younger than patients with angiographically proven obstructive coronary
lesions (p less than 0,001), and did not exhibit a rise in coronary risk
factors. These results suggest that in some cases myocardial infarction
is due to acute, completely reversible occlusion or severe stenosis of
larger coronary arteries without morphological or functional defects of
coronary arteries detectable later on.
http://www.ncbi.nlm.nih.gov/pubmed/10663915
Z Kardiol. 2000 Jan;89(1):36-42.
[Acute myocardial infarction in patients with angiographically normal
coronary arteries: clinical features and medium term follow-up].
[Article in German] Meierhenrich R1, Carlsson J, Brockmeier J, Miketic S, Sorges E, Tebbe U.
Author information 1Universitätsklinik für Anästhesiologie, Klinikum der Universität Ulm, Steinhövelstr. 9, D-89075 Ulm.
------------------------------
-
collateral circulation
http://www.ncbi.nlm.nih.gov/pubmed/2943529
Circulation. 1986 Sep;74(3):469-76.
Limitation of myocardial ischemia by collateral circulation during
sudden controlled coronary artery occlusion in human subjects: a
prospective study.
Cohen M, Rentrop KP.
We have shown
improvement in collateral filling immediately after sudden controlled
coronary occlusion in human subjects undergoing elective coronary
angioplasty. It has been suggested but not proved that collateral
circulation can limit myocardial ischemia. We prospectively studied 23
patients with isolated left anterior descending (n = 14) or right
coronary (n = 9) disease and normal left ventriculograms during elective
coronary angioplasty. A second arterial catheter was used for injection
of the contralateral artery to assess collateral filling before balloon
placement and during coronary occlusion by balloon inflation. Left
ventriculography was performed during another inflation. Grading of
collateral filling was as follows: 0 = none, 1 = filling of side
branches only, 2 = partial filling of the epicardial segment, 3 =
complete filling of the epicardial segment. Indexes of myocardial
ischemia included percent of the left ventricular perimeter showing new
hypocontractility and the sum of ST segment elevation measured on a
simultaneous 12-lead electrocardiogram recorded during each inflation.
Collateral filling during balloon occlusion and indexes of ischemia were
assessed at 30 to 40 sec into inflation. Aortic pressure and heart rate
did not correlate with the percent hypocontractile perimeter nor the
sum of ST segment elevation. There was a significant correlation between
the grade of collateral filling during inflation and both percent
hypocontractile perimeter (r = -.85) and the sum of ST segment elevation
(r = -.87). Anginal pain occurred in all patients with grade 0 or 1
collateral filling but in only 36% of patients with grade 2 or 3
collaterals. In conclusion, collateral circulation limits myocardial
ischemia as assessed by the extent of new ventricular asynergy and
electrocardiographic changes during coronary occlusion in patients.
free full text
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3689049/
http://www.ncbi.nlm.nih.gov/pubmed/23735225
BMC Med. 2013 Jun 4;11:143. doi: 10.1186/1741-7015-11-143.
The collateral circulation of the heart.
Meier P1, Schirmer SH, Lansky AJ, Timmis A, Pitt B, Seiler C.
The coronary arteries have been regarded as end arteries for decades.
However, there are functionally relevant anastomotic vessels, known as
collateral arteries, which interconnect epicardial coronary arteries.
These vessels provide an alternative source of blood supply to the
myocardium in cases of occlusive coronary artery disease. The relevance
of these collateral arteries is a matter of ongoing debate, but
increasing evidence indicates a relevant protective role in patients
with coronary artery disease. The collateral circulation can be assessed
by different methods; the gold standard involves intracoronary pressure
measurements. While the first clinical trials to therapeutically induce
growth of collateral arteries have been unavailing, recent pilot
studies using external counterpulsation or growth factors such as
granulocyte colony stimulating factor (G-CSF) have shown promising
results.
http://www.ncbi.nlm.nih.gov/pubmed/19897461
Heart. 2010 Feb;96(3):202-7. doi: 10.1136/hrt.2009.184507. Epub 2009 Nov 5.
Coronary collateral growth by external counterpulsation: a randomised controlled trial.
Gloekler S1, Meier P, de Marchi SF, Rutz T, Traupe T, Rimoldi SF, Wustmann K, Steck H, Cook S, Vogel R, Togni M, Seiler C.
The efficacy of external counterpulsation (ECP) on coronary collateral
growth has not been investigated in a randomised controlled study.
Objective To test the hypothesis that ECP augments collateral function
during a 1 min coronary balloon occlusion.
PATIENTS AND METHODS:
Twenty patients with chronic stable coronary artery disease were
studied. Before and after 30 h of randomly allocated ECP (20 90 min
sessions over 4 weeks at 300 mm Hg inflation pressure) or sham ECP (same
setting at 80 mm Hg inflation pressure), the invasive collateral flow
index (CFI, no unit) was obtained in 34 vessels without coronary
intervention. CFI was determined by the ratio of mean distal coronary
occlusive pressure to mean aortic pressure with central venous pressure
subtracted from both. Additionally, coronary collateral conductance
(occlusive myocardial blood flow per aorto-coronary pressure drop) was
determined by myocardial contrast echocardiography, and brachial artery
flow-mediated dilatation was obtained.
RESULTS: CFI changed from
0.125 (0.073; interquartile range) at baseline to 0.174 (0.104) at
follow-up in the ECP group (p=0.006), and from 0.129 (0.122) to 0.111
(0.125) in the sham ECP group (p=0.14). Baseline to follow-up change of
coronary collateral conductance was from 0.365 (0.268) to 0.568 (0.585)
ml/min/100 mm Hg in the ECP group (p=0.072), and from 0.229 (0.212) to
0.305 (0.422) ml/min/100 mm Hg in the sham ECP group (p=0.45). There was
a correlation between the flow-mediated dilatation change from baseline
to follow-up and the corresponding CFI change (r=0.584, p=0.027).
CONCLUSIONS: ECP appears to be effective in promoting coronary
collateral growth. The extent of collateral function improvement is
related to the amount of improvement in the systemic endothelial
function.
http://www.ncbi.nlm.nih.gov/pubmed/3318503
Am J Physiol. 1987 Nov;253(5 Pt 2):H1279-88.
Development of coronary collateral circulation in left circumflex
Ameroid-occluded swine myocardium. Roth DM1, Maruoka Y, Rogers J, White
FC, Longhurst JC, Bloor CM.
Coronary collateral development was
examined in 34 pigs after gradual occlusion of the left circumflex
coronary artery (LCX) with an Ameroid constrictor. Collateral
development was assessed by measurements of myocardial blood flow and
regional myocardial function at rest and during exercise over a 16-wk
period after placement of the constrictor. Coronary collateral
development was adequate to prevent severe infarction and restore blood
flow to the collateral-dependent LCX region within 3-7 wk. Infarction
averaged 5.0 +/- 1.3% of the LCX region. Blood flows at rest were 1.05
+/- 0.14 and 1.13 +/- 0.15 ml.min-1.g-1 in the subendocardium of the
collateral and control regions, respectively, 7 wk postoperatively.
Concurrently, collateral vessel development supported normal myocardial
function at rest as determined by systolic wall thickening in the LCX
region. However, collateral development was limited, since blood flows
during moderate and severe exercise were reduced in the LCX region
compared with control and left anterior descending and right coronary
regions. Blood flow ratios (collateral/control flow) during severe
exercise 3 wk postoperatively were 0.23 +/- 0.03 and 0.57 +/- 0.05 in
the subendocardium and subepicardium and were constant throughout the
16-wk period throughout the study. Myocardial function of the collateral
region also was reduced during exercise and a 30-min recovery period.
We suggest that this limited coronary collateral circulation, which
develops in response to gradual coronary occlusion in swine, serves as a
model for the human collateral circulation for the study of protocols
to alter growth and development of coronary collateral vessels.
==============================
http://www.ncbi.nlm.nih.gov/pubmed/11254922
Atherosclerosis. 2001 Apr;155(2):499-508.
Coronary atherosclerosis in unheralded sudden coronary death under age
50: histo-pathologic comparison with 'healthy' subjects dying out of
hospital. Schmermund A1, Schwartz RS, Adamzik M, Sangiorgi G, Pfeifer
EA, Rumberger JA, Burke AP, Farb A, Virmani R.
sudden coronary
death (SCD) in older individuals is generally associated with extensive
coronary atherosclerosis, although it may be the first manifestation of
ischaemic heart disease. In younger age-groups, SCD may occur in the
presence of less severe disease. We sought to (1) examine the extent of
coronary atherosclerosis in young victims of SCD compared with age- and
sex-matched controls, (2) analyse the composition of atherosclerotic
plaques in these patients, (3) identify the predominant mechanism of
SCD, and (4) evaluate the possibility of detecting this mechanism on the
basis of morphologic plaque features, in particular presence and amount
of lipid accumulation and calcific deposits.
METHODS AND RESULTS:
coronary
arteries were obtained at autopsy from 28 victims of SCD under age 50
with no prior clinical manifestation of ischaemic heart disease (IHD)
and no myocardial scar formation and from 16 age- and sex-matched
subjects dying of noncardiac causes out of hospital. Sections of all
available major coronary arteries were cut in 5-mm intervals to yield a
total of 1357 histologic sections, which were analysed using digitised
planimetry. Victims of SCD had significantly more major coronary
arteries per subject with luminal area narrowing > or = 75% than
controls (on average, 2.1 vs. 0.2). Plaque area per histologic section
was 5.1 +/- 2.1 mm(2) in SCD cases and 2.0 +/- 0.9 mm(2) in controls (P
< 0.001). The major constituent of all plaques was fibrous tissue.
Lipid core area per section was 0.49 +/- 0.59 mm(2) in SCD cases and
0.004 +/- 0.01 mm(2) in controls (P < 0.001), and calcified plaque
area was 0.18 +/- 0.19 mm(2) in SCD cases and 0.02 +/- 0.05 mm(2) in
controls (P < 0.001), both defining significant differences between
SCD cases and controls. Arterial thrombosis, most often with underlying
plaque rupture was the mechanism of SCD in > 80% of the cases.
Considering histologic sections with > or = 50 and with > or = 75%
area stenosis, plaque rupture was independently predicted by lipid core
area. Calcific deposits were a frequent feature of plaque rupture but
were only associated with it in univariate analysis.
CONCLUSIONS:
the
extent and severity of coronary atherosclerosis in young victims of SCD
as the first manifestation of IHD was substantially greater than in
age-and sex-matched controls and comparable with that previously
reported in SCD cases with a broader age range. Lipid core and calcified
plaque areas provided for excellent separation between the two groups,
which may have implications for identifying persons at increased risk
for SCD by non invasive visualisation and assessment of the coronary
arteries.
zzzz
http://europace.oxfordjournals.org/content/15/5/742.abstract.html
Heart rate variability and first cardiovascular event in populations
without known cardiovascular disease: meta-analysis and dose–response
meta-regression
Stefanie Hillebrand1,*, Karin B. Gast1,2,
Renée de Mutsert1, Cees A. Swenne3, J. Wouter Jukema3, Saskia
Middeldorp4, Frits R. Rosendaal1 and Olaf M. Dekkers1,5
+
Author Affiliations 1Department of Clinical Epidemiology, Leiden
University Medical Centre, Albinusdreef 2, 2333 ZA Leiden, The
Netherlands
Aims Heart rate variability (HRV) is associated with
cardiovascular disease (CVD) in individuals with known CVD. It is less
clear whether HRV is associated with a first cardiovascular event.
Therefore, we performed a meta-analysis to study the association between
HRV and incident cardiovascular events in populations without known
CVD.
Methods and results We performed a meta-analysis and
dose–response meta-regression of studies assessing the association
between HRV and CVD. We searched Pubmed, Embase, Web of Science,
Cochrane library, ScienceDirect, and CINAHL up to December 2011 for
eligible studies. We selected studies that used the standard deviation
of the normalized N–N interval (SDNN), low-frequency (LF) or
high-frequency (HF) spectral component as a measure of HRV. Primary
outcomes were (non)fatal cardiovascular events. Eight studies with a
total number of 21 988 participants were included. The pooled relative
risk (RR) comparing the lowest level to the highest level of SDNN was
1.35 (95% CI 1.10, 1.67). The pooled RRs for LF and HF were 1.45 (95% CI
1.12, 1.87) and 1.32 (95% CI 0.96, 1.81), respectively. In a
meta-regression, the predicted RR of incident CVD of the 10th and 90th
HRV (SDNN) percentiles compared with the 50th percentile were 1.50 (95%
CI 1.22, 1.83) and 0.67 (95% CI 0.41, 1.09).
Conclusion In
conclusion, low HRV is associated with a 32–45% increased risk of a
first cardiovascular event in populations without known CVD. An increase
in SDNN of 1% results in an ∼1% lower risk of fatal or non-fatal CVD.
http://www.ncbi.nlm.nih.gov/pubmed/9125996 free full
Am J Epidemiol. 1997 Apr 15;145(8):696-706.
Cardiac autonomic function and incident coronary heart disease: a
population-based case-cohort study. The ARIC Study. Atherosclerosis Risk
in Communities Study.
Liao D1, Cai J, Rosamond WD, Barnes RW, Hutchinson RG, Whitsel EA, Rautaharju P, Heiss G.
Cardiac autonomic activity, as assessed by heart rate variability, has
been found to be associated with postmyocardial infarction mortality,
sudden death, and all-cause mortality. However, the association of heart
rate variability and the incidence of coronary heart disease (CHD) is
not well described. The authors report on the association of baseline
cardiac autonomic activity (1987-1989) with incident CHD after 3 years
(1990-1992) of follow-up of the Atherosclerosis Risk in Communities
Study cohort selected from four study centers in the United States by
using a case-cohort design. The authors examined 137 incident cases of
CHD and a stratified random sample of 2,252 examinees free of CHD at
baseline. Baseline, supine, resting beat-to-beat heart rate data were
collected. High- (0.16-0.35 Hz) and low- (0.025-0.15 Hz) frequency
spectral powers and high-/low-frequency power ratio, estimated from
spectral analysis, and standard deviation of all normal R-R intervals,
calculated from time domain analysis, were used as the conventional
indices of cardiac parasympathetic, sympatho-parasympathetic, and their
balance, respectively. Incident CHD was defined as hospitalized
myocardial infarction, fatal CHD, or cardiac revascularization
procedures during 3 years of follow-up. The age, race, gender, and other
CHD risk factor-adjusted relative risks (and 95% confidence intervals)
of incident CHD comparing the lowest quartile with the upper three
quartiles of high-frequency power, low-frequency power,
high-/low-frequency power ratio, and standard deviation of R-R intervals
were 1.72 (95% confidence interval (CI) 1.17-2.51), 1.09 (95% CI
0.72-1.64), 1.25 (95% CI 0.84-1.86), and 1.39 (95% CI 0.94-2.04),
respectively. The findings from this population-based, prospective study
suggest that altered cardiac autonomic activity, especially lower
parasympathetic activity, is associated with the risk of developing CHD.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1216757/
Br Heart J. Sep 1989; 62(3): 165–170.
PMCID: PMC1216757
Cardiac parasympathetic activity during the early hours of acute myocardial infarction.
D McAreavey, J M Neilson, D J Ewing, and D C Russell
Cardiac parasympathetic activity was assessed in 21 patients during the
first 24 hours of acute myocardial infarction by measuring abrupt beat
by beat changes in RR interval, which are expressed as "RR counts".
Eleven patients had inferior wall infarction and 10 had anterior wall
myocardial infarction. The whole recording period was analysed in 11
patients (five inferior and six anterior), and intermittent hourly
periods were analysed in all 21 subjects. Mean RR counts were
significantly lower in patients with anterior than inferior infarction,
and below the normal range. Although mean heart rates were faster in the
group with anterior infarction, there was a dissociation between RR
counts and mean heart rate that was consistent with RR interval
variability being an independent measure of parasympathetic activity.
This study indicates that cardiac parasympathetic activity during acute
myocardial infarction can be simply and reliably assessed from
continuous electrocardiographic recordings, and it showed significantly
lower cardiac parasympathetic activity in patients with anterior
infarction.
Collaterals
http://www.ncbi.nlm.nih.gov/pubmed/23716567
Heart. 2013 Aug;99(15):1100-5. doi: 10.1136/heartjnl-
2013-304006. Epub 2013 May 28.
Clinical parameters associated with collateral development in patients with chronic total coronary occlusion.
van der Hoeven NW1, Teunissen PF, Werner GS, Delewi R, Schirmer SH,
Traupe T, van der Laan AM, Tijssen JG, Piek JJ, Seiler C, van Royen N.
Well-developed collaterals provide survival benefit in patients with
obstructive coronary artery disease (CAD). Therefore, in this study we
sought to determine which clinical variables are associated with
arteriogenesis.
DESIGN: Clinical and laboratory variables were
collected before percutaneous coronary intervention. Multivariate
analysis was performed to determine which variables are associated with
the collateral flow index (CFI).
PATIENTS: Data from 295 chronic
total occlusion (CTO) patients (Bern, Switzerland, Amsterdam, the
Netherlands and Jena, Germany) were pooled. In earlier studies, patients
had varying degrees of stenosis. Therefore, different stages of
development of the collaterals were used. In our study, a unique group
of patients with CTO was analysed.
INTERVENTIONS: Instead of
angiography used earlier, we used a more accurate method to determine
CFI using intracoronary pressure measurements. CFI was calculated from
the occlusive pressure distal of the coronary lesion, the aortic
pressure and central venous pressure.
RESULTS: The mean CFI was 0.39
± 0.14. After multivariate analysis, β blockers, hypertension and
angina pectoris duration were positively associated with CFI (B:
correlation coefficient β=0.07, SE=0.03, p=0.02, B=0.040, SE=0.02,
p=0.042 and B=0.001, SE=0.000, p=0.02). Furthermore also after
multivariate analysis, high serum leucocytes, prior myocardial
infarction and high diastolic blood pressure were negatively associated
with CFI (B=-0.01, SE=0.005, p=0.03, B=-0.04, SE=0.02, p=0.03 and
B=-0.002, SE=0.001, p=0.011).
CONCLUSIONS: In this unique cohort,
high serum leucocytes and high diastolic blood pressure are associated
with poorly developed collaterals. Interestingly, the use of β blockers
is associated with well-developed collaterals, shedding new light on the
potential action mode of this drug in patients with CAD.
http://www.ncbi.nlm.nih.gov/pubmed/20534067
Eur J Clin Invest. 2010 May;40(5):465-76. doi: 10.1111/j.1365-2362.2010.
02282.x.
The human coronary collateral circulation.
Seiler C.
Coronary collaterals are an alternative source of blood supply to
myocardium jeopardized by ischaemia. Well-developed coronary collateral
arteries in patients with coronary artery disease (CAD) mitigate
myocardial infarcts and improve survival.
METHODS AND RESULTS:
Collateral arteries preventing myocardial ischaemia during brief
vascular occlusion are present in 1/3 of patients with CAD. Among
individuals without relevant coronary stenoses, there are preformed
collateral arteries preventing myocardial ischaemia in 20-25%.
Collateral flow sufficient to prevent myocardial ischaemia during
coronary occlusion amounts to double dagger25% of the normal flow
through the open vessel. Myocardial infarct size, the most important
prognostic determinant after such an event, is the product of coronary
artery occlusion time, area at risk for infarction and the inverse of
collateral supply. Coronary collateral flow can be assessed only during
vascular occlusion of the collateral-receiving artery. The gold standard
for coronary collateral assessment is the measurement of intracoronary
occlusive pressure- or velocity-derived collateral flow index expressing
collateral as a fraction of flow during vessel patency. Approximately
one of five patients with CAD cannot be revascularized by percutaneous
coronary intervention or coronary artery bypass grafting. Therapeutic
promotion of collateral growth is a valuable treatment strategy in those
patients.
CONCLUSIONS: Promotion of collateral growth should aim at
inducing the development of large conductive collateral arteries (i.e.
arteriogenesis) and not so much the sprouting of capillary like vessels
(i.e. angiogenesis). Large conductive collateral arteries appear to be
effectively promoted via the activation of monocytes/macrophages by
means of granulocyte-colony stimulating factor or of augmenting coronary
flow velocity.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1277094/
Br Heart J. Feb 1987; 57(2): 139–143.
PMCID: PMC1277094
Importance of angina for development of collateral circulation.
M Fujita, S Sasayama, A Ohno, H Nakajima, and H Asanoi
The extent of collateral circulation in 46 patients who had
intracoronary thrombolysis within six hours of the onset of acute
myocardial infarction was evaluated. Patients who had had a previous
myocardial infarction (4 cases) or who had spontaneously recanalized
infarct related coronary arteries (5 cases) were excluded from the
analysis. Collateral development was graded during coronary
cineangiography according to the extent of opacification of the
collateral and epicardial arteries distal to the site of occlusion
(collateral index 0 to 3). Angina was considered to be present before
myocardial infarction if it had occurred more than one week before acute
myocardial infarction. Collateral channels were visible in only two of
19 patients without angina before infarction and nine of the 18 patients
with angina before infarction. The prevalence of angina and the
collateral index were not significantly influenced by the extent of
coronary vessel disease. It is concluded that myocardial ischaemia is
important in promoting collateral development in man as well as in
laboratory animals.
http://www.ncbi.nlm.nih.gov/pubmed/16570533
J Cardiol. 2006 Mar;47(3):115-21.
[Effect of collateral circulation on myocardial protection in patients
with acute myocardial infarction: comparison of
technetium-99m-tetrofosmin myocardial single photon emission computed
tomography and coronary angiography].
[Article in Japanese]
Yoshida M1, Kondo M, Abe Y, Kubota T, Matsuoka R, Araki M, Tanio H, Doyama K.
Evaluation of myocardial blood flow from collateral vessels into the
infarct area has been estimated by coronary angiography. In patients
with acute myocardial infarction with Thrombolysis in Myocardial
Infarction (TIMI) 0 flow, myocardial tracer uptake on single photon
emission computed tomography (SPECT) images can predict the collateral
blood flow in the infarct area if technetium (Tc)-99m-tetrofosmin was
administered before recanalization. The present study investigated
whether collateral blood flow evaluated by myocardial scintigraphy is a
good predictor of myocardial salvage in patients with acute myocardial
infarction.
METHODS:The study group consisted of 30 patients (mean
age 65 +/- 14 years, 23 males, 7 females) with first acute myocardial
infarction and coronary angiography evidence of total occlusion (TIMI 0)
within 12 hr after the onset. All patients had one vessel disease
related to infarction and TIMI 3 flow after percutaneous coronary
intervention (PCI). Tc-99m-tetrofosmin was injected intravenously before
the PCI. The regional severity score index (RSSI) was obtained from
SPECT using the 17 segment method with the four-point scoring system.
Myocardial viability was evaluated by the RSSI obtained from
thallium-glucose-insulin infusion SPECT after 1 week and regional wall
motion score index obtained from echocardiography during the chronic
phase.
RESULTS:The patients were divided into two groups according
to the angiographic collateral finding. There were no differences in
RSSI on thallium-glucose-insulin SPECT and regional wall motion score
between the good collateral group (n = 8) and poor collateral group (n =
22). Myocardial Tc-99m-tetrofosmin RSSI was similar in these groups. On
the other hand, the patients were divided according to
Tc-99m-tetrofosmin scintigraphic evaluation before PCI. RSSI on
thallium-glucose-insulin SPECT was significantly greater (0.7 +/- 0.5 vs
1.5 +/- 0.4, p < 0.01) and regional wall motion score was
significantly less (1.46 +/- 0.50 vs 2.08 +/- 0.78, p < 0.05) in the
lower Tc-99m-tetrofosmin RSSI (< 1.9) group (n = 22) compared with
the higher RSSI (> or = 1.9) group (n = 8). In addition, a
significant correlation was obtained between Tc-99 m-tetrofosmin RSSI
and regional wall motion score index (r = 0.53, p < 0.01).
CONCLUSIONS:The collateral flow evaluated by scintigraphy was significantly correlated with myocardial viability.
Dog Lab
http://www.ncbi.nlm.nih.gov/pubmed/1253370
Circulation. 1976 Mar;53(3 Suppl):I57-62.
Influence of collateral flow on the ischemic tolerance of the heart following acute and subacute coronary occlusion.
Schaper W, Pasyk S.
Acute occlusion of the circumflex branch of the left coronary artery
was produced in chronically instrumented conscious dogs. Tracer
microspheres were used to measure during an established time period, the
distribution of collateral flow within the infarcting myocardium. For
up to 2 hours after coronary occlusion the amount and distribution of
the collateral flow remained unchanged. Two to 4 hours after coronary
occlusion the subendocardial flow fell to almost zero and the
subepicardial flow rose. Between 6 and 48 hours subepicardial and total
collateral flow rose markedly. A no-reflow phenomenon is responsible for
the decline of collateral flow in the subendocardium. Evidence for this
hypothesis was provided by releasing the artery 1,2, 4 and 6 hours
after occlusion. The amount of subendocardium that could not be
reperfused was small after 1 hour and large after 6 hours of occlusion.
When the total collateral flow was very low, the subepicardium was not
able to be reperfused and a transmural myocardial infarction developed.
We conclude that the time delay between onset of ischemia and the
appearance of a no-reflow phenomenon depends upon the amount of
collateral flow. The occurrence of a no-reflow phenomenon in the
subendocardium increases the amount of flow to the subepicardium which
increases its chances of survival. Beyond the sixth hour after occlusion
the total amount of collateral flow increases which is interpreted as a
reduction of collateral resistance by passive caliber changes of the
collateral vessels. DNA-synthesis that signal active caliber changes
through cellular proliferation were always detected 24 hours after
complete occlusion of a coronary artery regardless whether the time
between onset of stenosis until complete occlusion was varied between 36
hours and 5 days. When the time to complete occlusion was 4 days,
myocardial infarction was prevented due to growth-transformation of
pre-existing collaterals. Four phases of collateral reactions in acute
coronary occlusion were observed: redistribution of available collateral
flow in favor of the subepicardium (t = 1 to 4 hours after occlusion),
2) increase of total collateral flow due to passive "stretch" of
collateral vessels (t = 4 to 24 hours after occlusion), 3) radial growth
of collateral vessels due to active cellular proliferation, (t = 24
hours to 5 days) 4) cellular proliferation to ensure a normal wall
thickness in growth'transformed collaterals (t = 5 days to 20 days after
coronary occlusion). In subacute coronary occlusion the first phase
does, of course, not apply.
Caridac Glyciosides
full pdf
Endogenous and exogenous cardiac glycosides: their roles in hypertension,
salt metabolism, and cell growth
Wilhelm Schoner and Georgios Scheiner-Bobis
Institute of Biochemistry and Endocrinology, Justus Liebig University Giessen, Giessen, Germany
full pdf
Semin Nephrol. 2005 Sep;25(5):343-51.
Endogenous cardiac glycosides: hormones using the sodium pump as signal transducer.
Schoner W1, Scheiner-Bobis G.
The search for an endogenous digitalis has led to the identification of
the cardenolides ouabain and digoxin and the bufadienolide
marinobufagenin in mammalian tissues and biological fluids. Ouabain's
release from adrenal glands is under the control of epinephrine and
angiotensin II; hence, its blood concentration changes rapidly on
physical exercise. It also is controlled by brain areas sensing
cerebrospinal Na+ concentration and apparently the body's K+ content
because urinary K+ loss leads to an increase in its plasma concentration
as well. Long-term treatment of rats with ouabain results in arterial
hypertension, and 50% of Caucasians with low-renin hypertension have
increased plasma concentrations of this cardenolide. Levels of digoxin,
which is synthesized from acetate in adrenal glands, increase slightly
in blood on prolonged exercise. It counteracts the hypertensinogenic
action of ouabain in rats, as does the ouabain antagonist PST 2238. The
plasma concentration of the bufadienolide marinobufagenin is increased
after cardiac infarction. It may show natriuretic properties because it
inhibits the alpha1 isoform of Na+/K+-adenosine triphosphatase (ATPase),
the main sodium pump isoform of the kidney, much better than other
sodium pump isoforms. These effects of endogenous cardiac glycosides are
observed at concentrations that do not inhibit the sodium pump.
Apparently, Na+/K+-ATPase is used by these steroids as a signal
transducer to activate tissue proliferation, heart contractility,
arterial hypertension, and natriuresis via various intracellular
signaling pathways.
http://www.ncbi.nlm.nih.gov/pubmed/17610345
Am J Cardiovasc Drugs. 2007;7(3):173-89.
Endogenous and exogenous cardiac glycosides and their mechanisms of action.
Schoner W1, Scheiner-Bobis G.
Cardiac glycosides have been used for decades to treat congestive heart
failure. The recent identification of cardiotonic steroids such as
ouabain, digoxin, marinobufagenin, and telocinobufagin in blood plasma,
adrenal glands, and hypothalamus of mammals led to exciting new
perspectives in the pathology of heart failure and arterial
hypertension. Biosynthesis of ouabain and digoxin occurs in adrenal
glands and is under the control of angiotensin II, endothelin, and
epinephrine released from cells of the midbrain upon stimulation of
brain areas sensing cerebrospinal Na(+) concentration and, apparently,
the body's K(+) content. Rapid changes of endogenous ouabain upon
physical exercise may favor the economy of the heart by a rise of
intracellular Ca(2)(+) levels in cardiac and atrial muscle cells.
According to the sodium pump lag hypothesis, this may be accomplished by
partial inhibition of the sodium pump and Ca(2+) influx via the
Na(+)/Ca(2+) exchanger working in reverse mode or via activation of the
Na(+)/K(+)-ATPase signalosome complex, generating intracellular calcium
oscillations, reactive oxygen species, and gene activation via nuclear
factor-kappaB or extracellular signal-regulated kinases 1 and 2.
Elevated concentrations of endogenous ouabain and marinobufagenin in the
subnanomolar concentration range were found to stimulate proliferation
and differentiation of cardiac and smooth muscle cells. They may have a
primary role in the development of cardiac dysfunction and failure
because (i) offspring of hypertensive patients evidently inherit
elevated plasma concentrations of endogenous ouabain; (ii) such elevated
concentrations correlate positively with cardiac dysfunction,
hypertrophy, and arterial hypertension; (iii) about 40% of Europeans
with uncomplicated essential hypertension show increased concentrations
of endogenous ouabain associated with reduced heart rate and cardiac
hypertrophy; (iv) in patients with advanced arterial hypertension,
circulating levels of endogenous ouabain correlate with BP and total
peripheral resistance; (v) among patients with idiopathic dilated
cardiomyopathy, high circulating levels of endogenous ouabain and
marinobufagenin identify those individuals who are predisposed to
progressing more rapidly to heart failure, suggesting that endogenous
ouabain (and marinobufagenin) may contribute to toxicity upon digoxin
therapy. In contrast to endogenous ouabain, endogenous marinobufagenin
may act as a natriuretic substance as well. It shows a higher affinity
for the ouabain-insensitive alpha(1) isoform of Na(+)/K(+)-ATPase of rat
kidney tubular cells and its levels are increased in volume expansion
and pre-eclampsia. Digoxin, which is synthesized in adrenal glands,
seems to counteract the hypertensinogenic action of ouabain in rats, as
do antibodies against ouabain, for example, (Digibind) and rostafuroxin
(PST 2238), a selective ouabain antagonist. It lowers BP in ouabain- and
adducin-dependent hypertension in rats and is a promising new class of
antihypertensive medication in humans.
Ouabain Study in Dog Lab - Benefits for Ischemic Myocardium
Ouabain_Dog_Vatner
CIRCULATION VOL 58, No 4, OCTOBER 1978
STEPHEN F. VATNER, M.D. AND HANK BAIG, M.S.E.E.
Comparison of the Effects of Ouabain and Isoproterenol on Ischemic Myocardium of Conscious Dogs.
Ouabain appeared to alleviate the ischemic condition
Jeffrey Dach MD
7450 Griffin Road Suite 190
Davie, Florida 33314
954-792-4663
http://www.jeffreydachmd.com
http://www.drdach.com/
http://www.naturalmedicine101.com/
http://www.truemedmd.com/
http://www.bioidenticalhormones101.com/
For Disclaimer:
Click Here
The reader is advised to discuss the comments on these pages with
his/her personal physicians and to only act upon the advice of his/her
personal physician. Also note that concerning an answer which appears as
an electronically posted question, I am NOT creating a physician —
patient relationship.
Although identities will remain confidential
as much as possible, as I can not control the media, I can not take
responsibility for any breaches of confidentiality that may occur.
Link to this article
Copyright (c) 2014 Jeffrey Dach MD All Rights Reserved
This article may be reproduced on the internet without permission,
provided there is a link to this page and proper credit is given.
FAIR
USE NOTICE: This site contains copyrighted material the use of which
has not always been specifically authorized by the copyright owner. We
are making such material available in our efforts to advance
understanding of issues of significance. We believe this constitutes a
‘fair use’ of any such copyrighted material as provided for in section
107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section
107, the material on this site is distributed without profit to those
who have expressed a prior interest in receiving the included
information for research and educational purposes.
Serving Areas
of: Hollywood, Aventura, Miami, Fort Lauderdale, Pembroke Pines,
Miramar, Davie, Coral Springs, Cooper City, Sunshine Ranches,
Hallandale, Surfside, Miami Beach, Sunny Isles, Normandy Isles, Coral
Gables, Hialeah, Golden Beach ,Kendall,sunrise, coral springs,
parkland,pompano, boca raton, palm beach, weston, dania beach, tamarac,
oakland park, boynton beach, delray,lake worth,wellington,plantation
 Hormone Disruption and Low Testosterone From Pain Pills by Jeffrey Dach MD
Hormone Disruption and Low Testosterone From Pain Pills by Jeffrey Dach MD




 ,
depression (BDI-II), and hematocrit levels showed improvement during
treatment, generally more so at the 7.5 mg/day dosage (P < .001 vs.
baseline for most parameters). Pain scores (BPI-SF) decreased slightly on
7.5 mg/day (interference score: P < .05 vs. baseline and 5 mg/day);
the use of opioids did not change appreciably. The testosterone patches
were generally well tolerated.
,
depression (BDI-II), and hematocrit levels showed improvement during
treatment, generally more so at the 7.5 mg/day dosage (P < .001 vs.
baseline for most parameters). Pain scores (BPI-SF) decreased slightly on
7.5 mg/day (interference score: P < .05 vs. baseline and 5 mg/day);
the use of opioids did not change appreciably. The testosterone patches
were generally well tolerated.
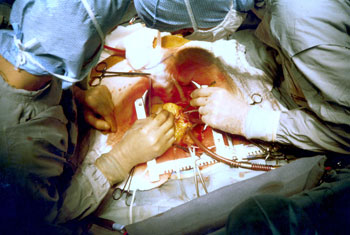
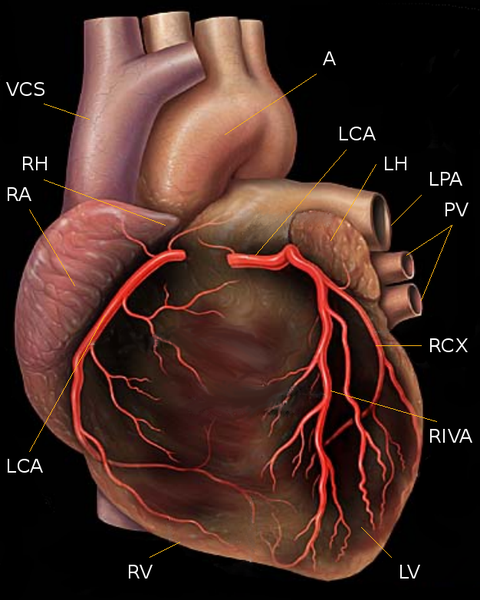

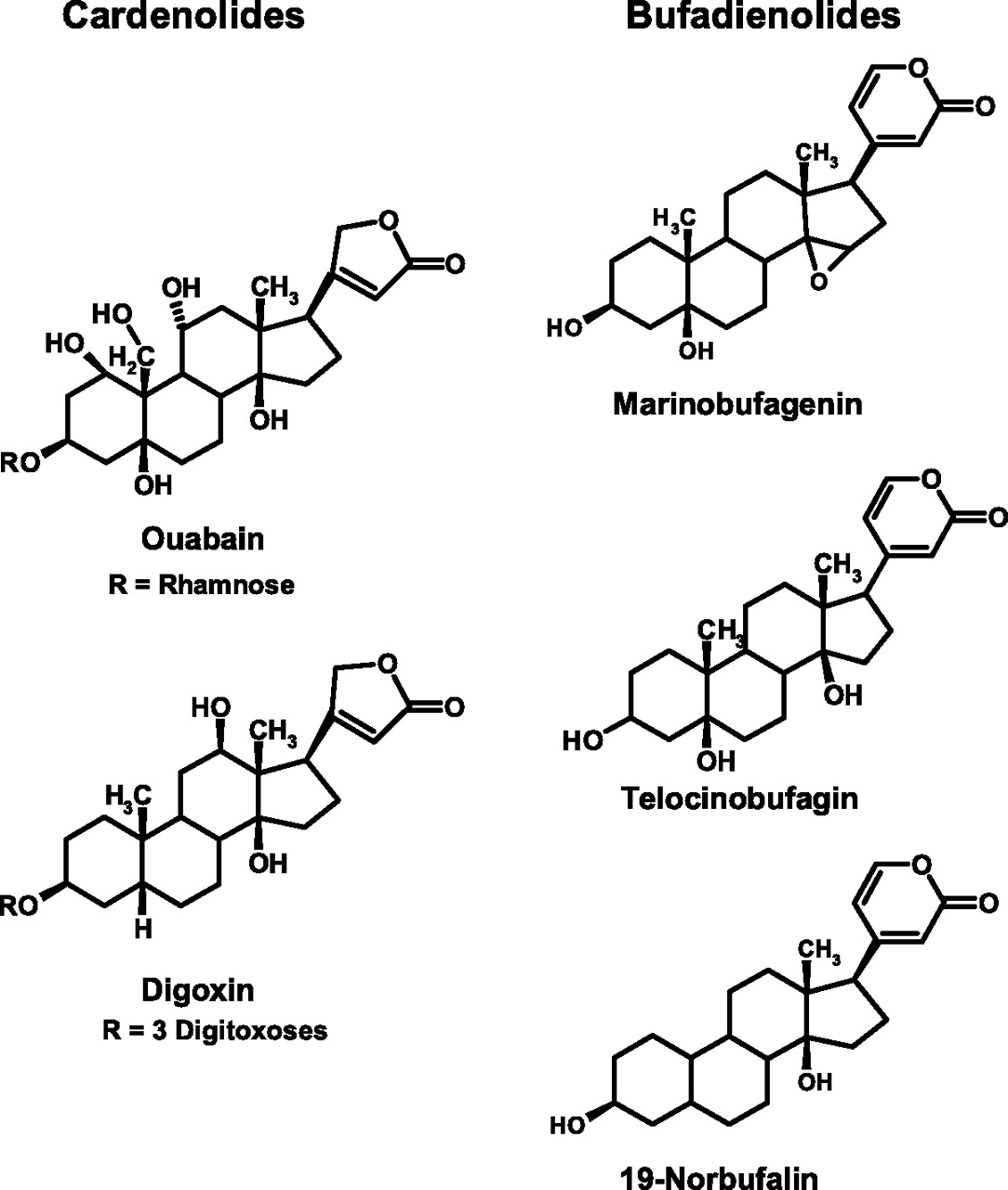
{kind=link}